When we are asked to help set up brand new practices, one of the first things we work on with our clients is strategy.
Sure, you could probably open a new optometry practice in the right location and get enough traffic to survive. But what if you want to do more than just survive? What if you want to thrive?
Aspiring owners should have Goals, Actions and Priorities as defined here:
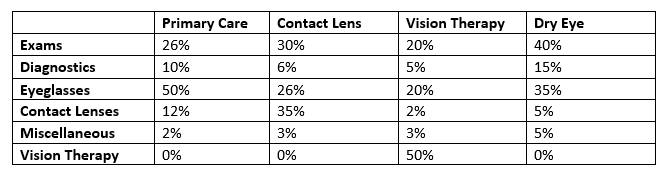
- Goals: Achieve a revenue, profit, or market share target. For example, achieve 10% of gross revenue through diagnostic testing.
- Actions: This outlines what needs to happen. This one can be as simple as “open a new office.”
- Priorities: Define areas of investment for time, resources, or capital for advancing the company, such as increasing brand awareness in digital channels.
While, Goals, Actions, and Priorities may help inform the creation of a strategy, they’re not equivalent to your strategy.
There are a number of things you need to consider in order to formulate a strategy. First, what are your strengths and passions? This will help you formulate your service and product offerings. Next, evaluate the landscape. Who else is offering a similar service? How will you create a unique experience to drive traffic to your location instead of theirs?
One of my favourite examples to illustrate how different strategies play out is the coffee shop. For most of us, we have a few different options when it comes to coffee. We may choose differently depending on the circumstance. For instance, if I am just grabbing a coffee to drink while driving, my go-to place is Tim Horton’s. If we have a client meeting, we often choose Starbucks for a more formal feel. If I am meeting friends and we decide to get a bite to eat, I choose the local coffee establishment that offers larger tables and a wider selection of lunch options.
How will you make the experience in your office different? Why will the consumer choose your office over someone offering similar services? You need a strategy.
 Roger Martin and A.G. Lafley provide an excellent framework in Playing To Win to help you define a strategy through answering five big questions:
Roger Martin and A.G. Lafley provide an excellent framework in Playing To Win to help you define a strategy through answering five big questions:
- What is our winning aspiration?
- Where will we play?
- How will we win?
- What capabilities must be in place?
- What management systems are required?
The answers to these questions will help you formulate your strategy. From there you can plan the steps to bring that strategy to life. Every decision should be evaluated against this strategy to ensure they are aligned.

KELLY HRYCUSKO
is the co-founder and managing partner of Simple Innovative Management Ideas (SIMI) Inc. and expert Practice Management contributor for Optik magazine. She can be reached at info@simiinc.com.
















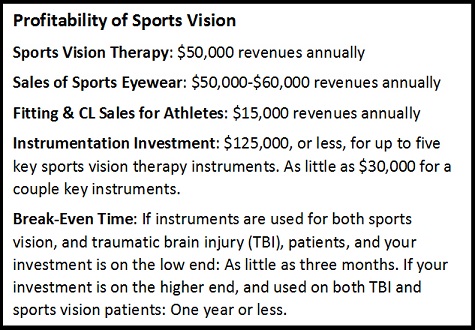 use most of these instruments, not only on our sports vision patients, but on our traumatic brain injury patients and developmental vision patients, so with the shared value, recouping the investment took us less than a year.
use most of these instruments, not only on our sports vision patients, but on our traumatic brain injury patients and developmental vision patients, so with the shared value, recouping the investment took us less than a year.