Canadian Eye Care Business Review is proud to announce that registration is now open for their first webinar; “The Future of Independent Optometry”. The webinar will be available live on Monday May 29th from 8 PM to 9PM EDT.
This format will provide optometrists across the country an opportunity to hear from a group of Canadian thought leaders on topics critical to the future of independent optometry.
Drs. Jeff and Tina Goodhew,
Co-Editors of Canadian Eye Care Business Review will host the webinar with the following panelists:
Dr. Daryan Angle
Executive Vice President Chairman of the Board, IRIS The Visual Group, Waterloo ON
Mr. Ken Barbet
Eye Recommend, Chief Executive Officer, Calgary AB,
Dr. Altaz Shajani
Practice Owner, North Vancouver BC
Dr. Sheldon Salaba
Practice Owner, Hamilton ON
Dr. Al Ulsifer
CEO and President, FYidoctors, Calgary AB
The questions that will be addressed include:
- What is the impact of supplier side consolidation on independent eye care?
- Why are independents selling out to larger groups? Fear or opportunity?
- What are the risks and opportunities in moving from retail to medical?
- How should independents create great customer experiences and loyalty?
- How do solo practitioners manage the risk in today’s environment?
We are excited to have a discussion such as this on a very important topic, one that is top of mind for many in the industry.
There is no-cost to register. Please reserve your virtual place by registering online:
We look forward to your active engagement.























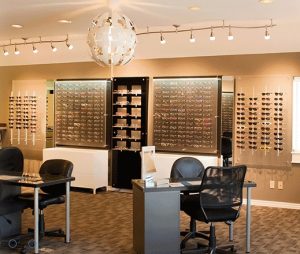
 djustments in plain sight to highlight your expertise in optics. If you’re designing or redesigning your store, consider having the lab clearly in view behind a window. Customers love behind the scenes peeks. Your clients will be delighted to see lenses edged on site and how you make each pair of eyeglasses specially to order.
djustments in plain sight to highlight your expertise in optics. If you’re designing or redesigning your store, consider having the lab clearly in view behind a window. Customers love behind the scenes peeks. Your clients will be delighted to see lenses edged on site and how you make each pair of eyeglasses specially to order.