
My office, a four-doctor practice in Cary, N.C., is dominated by Millennial patients, those born between 1982 and 2002. That means we’ve had to put thought into creating the kind of office that appeals to these young patients. 
We’ve had to understand what makes the Millennial patient different from patients of older generations, and the type of office environment they are likely to appreciate, return to for care and refer others to experience.
I’m a Millennial myself, and my staff is almost entirely Millennials, age 25-37, so we know from first-hand experience the kind of office environment that is likely to appeal to people our age.
Equip Exam Rooms with Large Screens for Patient Education
I have used iPad technology for charting in my exam room before, but have found having large desktop monitors to be better technology for Millennial patient education. We use multiple large screens to pull up high-quality images of retinal scans and meiboiman gland imaging for patient education, and it lets me review their prescriptions easily with them.
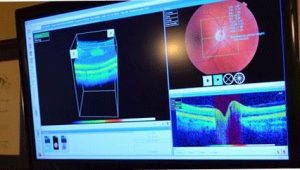 Millennials are invested in their personal care; they want to know what you changed and what you are writing in their chart. There is no diagnosis or concept that they feel is too complicated for them to understand, and they expect complete transparency. Large screens that they can easily see from the exam chair give them that feeling of being surrounded by state-of-the-art technology that they are actively a part of; not just me typing into a chart they can’t see.
Millennials are invested in their personal care; they want to know what you changed and what you are writing in their chart. There is no diagnosis or concept that they feel is too complicated for them to understand, and they expect complete transparency. Large screens that they can easily see from the exam chair give them that feeling of being surrounded by state-of-the-art technology that they are actively a part of; not just me typing into a chart they can’t see.
Offer Free Wi-Fi in Office
We have free WiFi, but to protect patient records, we have two separate accounts. We have a public WiFi access that patients can utilize, and a separate private WiFi account for staff and doctors that is password-protected. This protects us from the threats of viruses or potential identity theft issues, while still letting our patients enjoy a wireless internet connection, and have the experience they expect in a high-technology office.
Tell Patients Why They Should Buy from You: Technology & Value
Millennials are not shy to tell you they are buying online and they need you to supply the PD. There is no sense of shame in purchasing from outside your office, and they expect you to give them everything they need to do so. Instead of bashing Warby Parker, or other online stores, I explain how what I offer in my office differs from what an online retailer is able to offer.
I let them know that online stores don’t usually offer the kind of doctor-patient exchange that leads to pinpointing and prescribing the kind of technology we just discussed during their exam: the anti-fatigue lenses to combat their tired eyes, the blue-blocker glare coatings and tinted lenses to reduce their light sensitivity and frequent headaches, the low prism I showed them to relax their eye muscles. I usually say something like, “I understand having an inexpensive back-up pair that you don’t mind throwing around in a suitcase, or scratching up, but for the glasses you wear to work every day, you need much better technology if you want to your eyes seeing and feeling their best.”
Talking about all these new lens technologies in the exam takes a lot of chair time, but if I’m not offering them state of the art lens technology, then why would I expect them to think there is a difference between my glasses and Warby Parker’s? You have to prescribe and educate the difference for them to understand your glasses aren’t the same.
Dr. Lyerly says the type of “capsule” marketing shown in the above picture is more effective at marketing to Millennials than a traditional frame board display.
 Go from Frame Board to “Capsule”
Go from Frame Board to “Capsule”
We continually update the appearance of our optical to provide an attractive shopping experience. A clinical feel with racks of frame boards? Not what Millennials are looking for. You can tell by the clothing stores, restaurants and craft breweries (the epitome of how Millennials spend more for products they think are better quality), they spend money for the aesthetic that best captures and engages their interest.
We are working to turn traditional frame boards into capsules of brand stories where patients can get an idea of each frame line’s identity – what makes them different, where they are made and what social message they have. We want to present high-quality frames with a high-quality aesthetic, so right away when you enter the optical you can tell what’s inside is much nicer than what they can expect from discount stores or online warehouses.
The message is quality, performance, craftsmanship and technology right when you walk in, and before you even try on a frame!
Be Selfie-Friendly
We also want to make an environment where people want to take pictures and selfies. Bright lighting, clean lines, a coffee station, a bar height optical table – this is how we create a visual environment that a patient wants to share on their social media accounts. Nothing is better advertising than when a patient tags us in a post that they want to share with their friends, bragging about the frames or the experience they just had in our office.

JENNIFER LYERLY, OD
Jennifer Lyerly, OD, is an associate at Triangle Visions Optometry in Cary, N.C. To contact her: jelyerly@gmail.com









 Stuart J. Thomas, OD, is the owner of
Stuart J. Thomas, OD, is the owner of  Ellen Byrum-Goad, LDO, is practice manager. To contact:
Ellen Byrum-Goad, LDO, is practice manager. To contact: 







 OALS
OALS